Related Posts

Common Site-Level Mistakes in Healthcare Construction
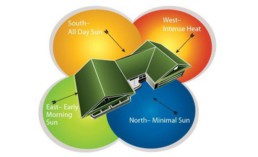
In healthcare construction, site decisions become clinical decisions. Orientation, drainage,…

Negative Pressure Rooms in Hospitals
Negative pressure rooms (NPRs) may occupy a small footprint in a hospital, but their performance…

Designing for Night-Shift Healthcare Workers
Hospitals run 24/7, but most design decisions are made with daytime workflows in mind. We’ve been…

The Science of Hospital Windows
Windows in hospitals do far more than bring in light; they influence recovery rates, infection…

How Design Impacts Patient Care
Ever wondered what goes into designing a hospital or clinic that truly works - for doctors, staff,…

Textures in Healthcare Spaces
When designing hospitals or clinics, texture is often seen as a “finishing touch.” At Shree…

The Lifecycle of a Healthcare Facility Design
Ever wondered what goes into designing a hospital or clinic that actually works - clinically,…

Designing NABH-Compliant Hospital Interiors
A well-designed hospital isn’t just about aesthetics. From fire safety and infection control to…

Blueprint for Healthcare Design
From room dimensions to lighting levels, every detail matters in healthcare design. At Shree…

Building Better Day Surgery Centres
Efficient care, happier patients, and smarter workflows - this is what defines a successful…

Designing Healthcare Spaces That Truly Heal
From concept to completion, every medical space we design prioritizes patient flow, staff…

The Business of Wellness
In the $1.8 trillion wellness industry, first impressions matter. Patients don’t just choose a…

Efficient Hospital and Clinic Design
India’s emerging cities are growing rapidly, creating an urgent demand for accessible and efficient…

Creating Calming and Confidential Spaces for Fertility Clinics
As the demand for fertility treatments grows, the architecture of these clinics plays a vital role…

Designing the Perfect Hospital Pharmacy
Hospital pharmacies are the backbone of seamless patient care. From efficient workflows to secure…

Preventive Care Facility Design Strategies
With preventive care emerging as the future of healthcare, this post outlines key architectural…

Thermal Comfort Decoded
Thermal comfort plays a critical role in patient recovery, staff productivity, and overall…

Building for Tomorrow: The Imperative of Adaptable Healthcare Design
Healthcare facilities need to be as dynamic as the industry itself. Traditional, rigid designs can…

Designing Single Speciality Healthcare Centres
As single-speciality centres grow, their design needs become more specific, calling for tailored…

Innovative Design Solutions for Senior Care Facilities
Designing senior-friendly spaces in healthcare facilities is crucial for catering to the evolving…

Designing a Dental Clinic for Success
Providing quality dental care is not just about the technical elements of the treatment. It's also…

3 Lessons Learned While Building a Cardiac Cath Lab
Cardiac care design is moving at the sound of a new beat! The number of Cath labs in India has…

5 Essential Elements of Healthcare Design
Design makes a significant impact on the delivery of care for both healthcare providers and…

5 Best Ways to Create Healing Spaces for Kids
Designing spaces in healthcare facilities tailor-made for children is a lesson in balance! A…

Top 5 Trends in Healthcare Design
Design can make all the difference when it comes to improving patient care. From a patient’s point…

The Architectural Design of Hospital Facilities
Shree Designs designed and executed many efficient and safe healthcare setups in the middle of the…

Dauntless Designers
Healthcare Radius in its 7th Anniversary Special issue in October 2019, featured a "power list of…

The changing face of healthcare design
After completing a decade in designing healthcare projects, Kshititi Nagarkar, principal architect,…
Thumb Rules for Planning and Designing of Hospitals
Traditional rules of thumb in healthcare planning have changed. Once-accepted rules can now be the…
